AUTHOR : Dentist Michał Godula
ABSTRACT: Congenital absence of tooth buds is an increasingly common abnormality. Agenesis is the result of disturbances in the early stages of tooth development. Treatment of patients with one or more missing tooth buds usually requires a comprehensive and complex treatment, ensuring optimal results over a long period of time.
KEY WORDS: hypodontia, anodontia, implants, prosthetic
ARTICLE PUBLISHED: October 7, 2022
Congenital absence of tooth buds is an increasingly common abnormality. Agenesis is the result of disorders in the early stages of tooth development. Treatment of patients with one or more missing tooth buds usually requires a comprehensive and complex treatment, ensuring optimal results over a long period of time.
Congenital absence of tooth buds is an increasingly common abnormality. Agenesis is the result of disorders in the initial stage of tooth development. Its etiology is multifactorial, but its development is most often influenced by genetic and environmental factors. It can occur as an independent form or as one of the symptoms of genetic syndromes. The highest percentage is observed in ectodermal dysplasia. In tooth agenesis, depending on their missing number, hypo-, oligo- and anodontia are distinguished. According to Ogaard and Krogstad, hypodontia is the absence of one to six teeth, oligodontia the absence of more than 6 teeth, and anodontia the complete absence of tooth buds. The occurrence of this anomaly ranges from 0.3 to 17.5% and is more common in females. In the permanent dentition, it most often affects the mandibular second premolars, upper lateral incisors, upper second premolars, and lower central incisors (1, 2, 3, 4, 5). Treatment of patients with one or more missing tooth buds usually requires a comprehensive and complex treatment that provides optimal results over a long period of time.
The aim of the study is to present the implantoprosthetic procedure in a patient with congenital absence of the upper left lateral incisor tooth bud.
Case description
A 20-year-old patient reported in April 2019 to the Specialist Dentistry Center in Żory to replace the missing tooth 22. An intraoral examination revealed the absence of the upper left lateral incisor and a shift of the symmetry axis of the upper dental arch to the left (Fig. 1, 2, 3). The interview revealed hypodontia of tooth 22. The patient was under orthodontic control in childhood, using a Schwarz plate to secure the space between teeth 21 and 23. For 4 years, she had been using a mini-denture to replace the missing tooth. After reaching skeletal maturity, she decided to have a permanent prosthetic restoration.
The patient was presented with two treatment plans using permanent prosthetic restorations. Each of them could have been preceded by orthodontic treatment to restore the disturbed symmetry and improve the aesthetics of the smile, but the patient did not consent to such preparatory procedure. In the first option, the patient was presented with the possibility of making a prosthetic bridge, mounted on pillars 21 and 23. The second, on the other hand, included implant prosthetic treatment. The patient decided to undergo implant prosthetic treatment.
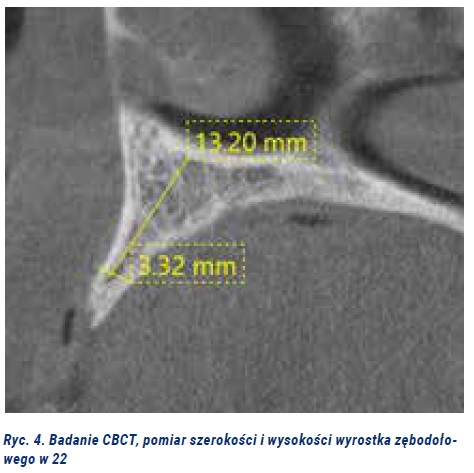
Before the implantation procedure, the bone and anatomical conditions were assessed based on computed tomography. The height and width of the alveolar process were determined to be 13.2 mm x 3.32 mm, respectively. It was found necessary to improve the mucosal-bone conditions. Under infiltration anesthesia, the alveolar process was augmented using the xenographic bone material Bio-Oss (Geistlich), the Bio-Gide membrane (Gestlich) and the Mesch titanium membrane.
At the follow-up visit, 7 days after the procedure, separation of part of the flap with exposure of the titanium membrane was noted. The membrane was removed and the mucosa was left to heal. At that time, the patient was provided with an adhesive bridge, filling the gap in tooth 22. After 3 months and complete healing of the mucosa, soft tissue augmentation was performed to thicken them and cover the recession on tooth 21 (2 mm). Under Ubistesin forte infiltration anesthesia, an incision was made between teeth 21 and 23 from the palatal side, as well as groove incisions in teeth 21 and 23. From the vestibular side, an incision was made to activate the envelope flap mesially and distally from teeth 21 and 23, with deepitelization of anatomical papillae. The interdentally divided flap was dissected in the buccal direction, with the incision parallel to the bone up to the mucogingival junction, and the flap was mobilized through a superficial and deep incision, which allowed for compensation of the tension during the coronal shift. A full-thickness flap was taken from the molar region on the left palate and deepithelialized. Two layers of connective tissue were sewn into the recipient site. One vertically into the interdental space, and the other horizontally, covering the root of tooth 21 and the area of 22. The wound was closed with 6.0 knot sutures in the palatal region of tooth 22. The papillae were closed with suspension sutures. The donor site on the palate was provided with sutures, collagen, and a dressing plate, prepared before the procedure. The sutures from the donor site were removed after 7 days and from the recipient site after 14 days. After two weeks, an adhesive bridge was again made to reconstruct the missing tooth 22.
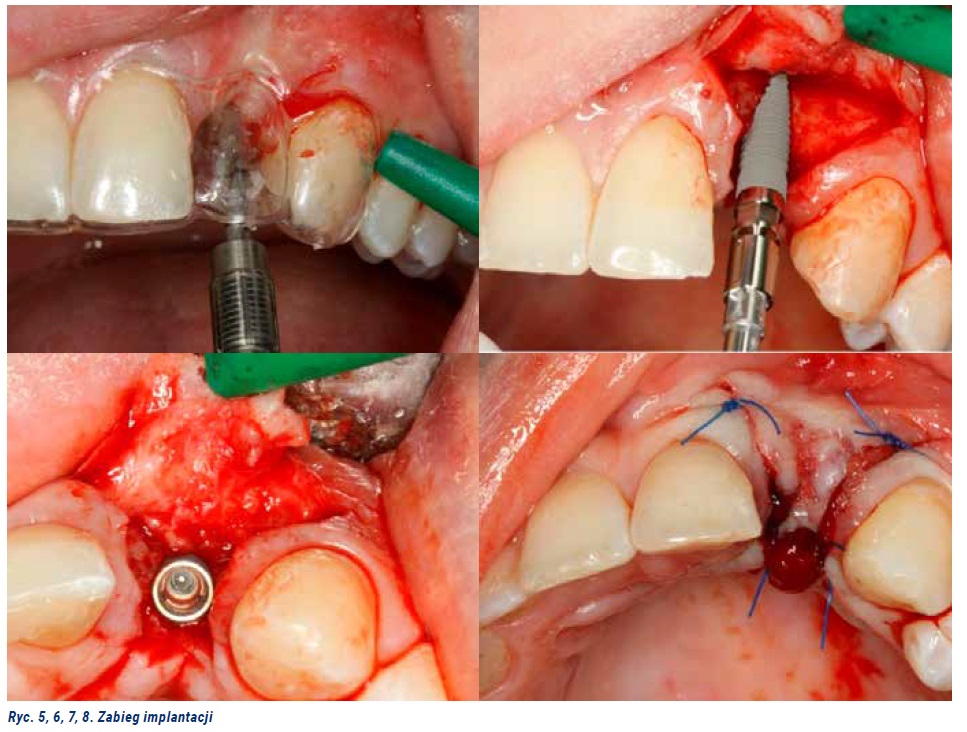
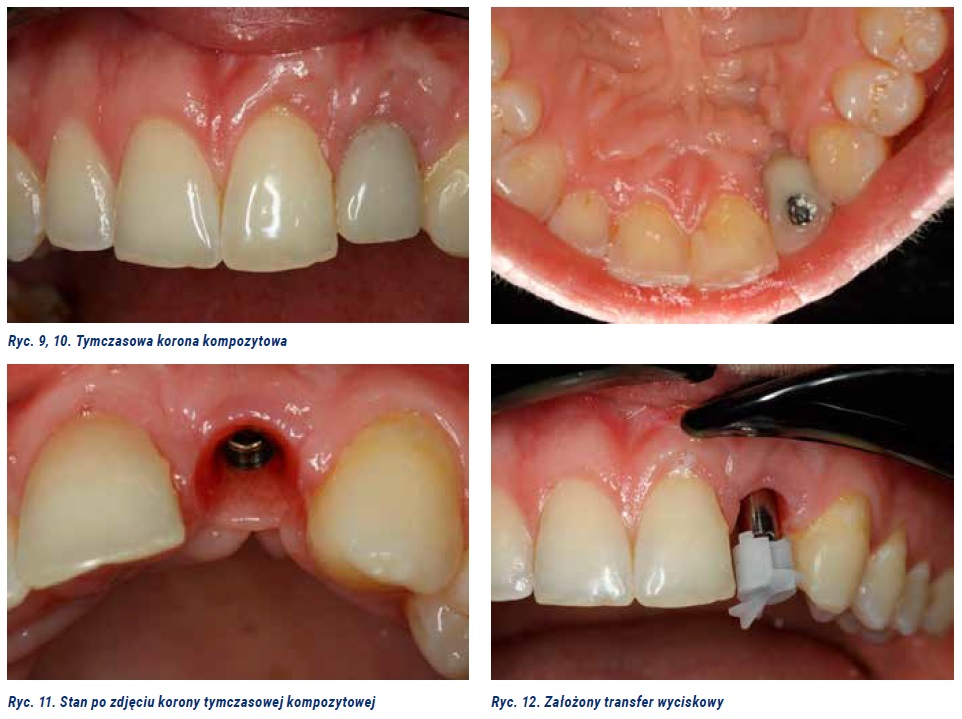
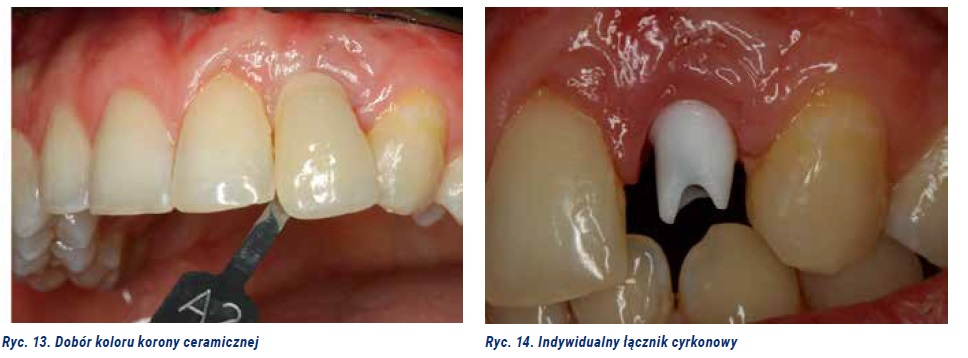
Twelve months later, another CT scan was performed, which showed an improvement in the dimensions of the alveolar process in the area of 22. The implantation procedure was started. The procedure was performed with the preparation of a full-thickness flap. A 3.3 x 11 mm ConeLock implant was implanted. The wound was sutured tightly (Fig. 5, 6, 7, 8). The implant was exposed 6 months after the implantation procedure. In order to obtain a favorable emergence profile, a temporary composite crown was made (Fig. 9, 10, 11). Four weeks later, an impression was taken for a ceramic crown with an individual zirconium abutment and the color of the future crown was selected (Fig. 12, 13, 14). The crown was placed on Ketac Cem glass ionomer cement (Fig. 15). The work performed met the patient's aesthetic expectations. The patient remains under constant dental supervision and returns for regular visits.
Summary
In the case of detection of hypodontia, preventive treatment at the developmental age is important, aimed at maintaining the space until the end of bone development, when it will be possible to use intraosseous implants. Maintaining the space is possible thanks to the use of removable or fixed orthodontic appliances and prosthetic restorations in the form of permitted removable partial dentures. An alternative to prosthetic treatment of congenital missing teeth is: orthodontic closing of the space after an uneducated tooth or autotransplantation of natural teeth. Autotransplantation is possible, however, only when there are specific donor possibilities (6, 7, 8). Therapeutic treatment in adult patients in whom hypodontia treatment has not been implemented earlier is definitely more complicated than in children or adolescents. In the described case, the patient remained under the care of an orthodontist from early childhood, thanks to which the reconstruction of the missing tooth 22 was not associated with long-term treatment. According to some authors, spaces in the anterior section of the maxilla should be closed orthodontically and, if necessary, space should be recreated in the lateral sections of the dental arch (9, 10). This is dictated by significantly lower aesthetic requirements than in the anterior section of the maxilla. Therefore, prosthetic rehabilitation of adult patients with hypodontia of the upper lateral incisors is a challenge for the doctor. It is important to ensure not only long-term stability, but above all to meet the patient's aesthetic requirements (11, 12, 13).
Bibliography
- Zadurska M., Siemińska−Piekarczyj B., Pietrzak-Bilińska B., Ratyński P., Salinger M.: Hypodontia – frequency, forms and symptoms based on the literature and our own material. Czas. Stomat. 1999, 52, 612–621.
- Zadurska M., Siemińska–Piekarczyk B., Pietrzak Bilińska B., Ratyński P., Salinger M.: Hypodontia– etiology based on the literature. Czas. Stomatol., 1999, LII, 2, 130-133.
- Al-ani AH, Antoun JS, Thomson WM, Merriman TR, Farella M: Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. BioMed Res Int 2017.
- Matalova E, Fleischmannova J, Sharpe PT, Tucker AS: Tooth agenesis: from molecular genetics to molecular dentistry, J Dent Res 2008; 7: 617-623.
- de Mezer M.: Hypodontia – views on occurrence and treatment. Pozn. Stomat. 2001, 28, 201–205.
- Szemraj-Folmer A, Kuc-Michalska M, Plakwicz P. Patient with asymmetric multiple hypodontia treated with autotransplantation of 2 premolars. Am J Orthod Dentofacial Orthop. 2019 Jan;155(1):127-134.
- Ko JM, Paik CH, Choi S, Baek SH. A patient with protrusion and multiple missing teeth treated with autotransplantation and space closure. Angle Orthod. 2014 May;84(3):561-7.
- Kafourou V, Tong HJ, Day P, Houghton N, Spencer RJ, Duggal M. Outcomes and prognostic factors that influence the success of tooth autotransplantation in children and adolescents. Dent Traumatol. 2017 Oct;33(5):393-399.
- Rosa M, Zachrisson BU: The space-closure alternative for missing maxillary lateral incisors: an update. J Clin Orthod 2010; 44: 540-549.
- Woodworth DA, Sinclair PM, Alexander RG: Bilateral congenital absence of maxillary lateral incisors: a craniofacial and dental cast analysis. Am J Orthod 1985; 87: 280-293.
- Singer SL, Henry PJ, Lander ID: A treatment planning classification for oligodontia. Int J Prosthod 2010; 23: 99-106.
- Rakhashan V: Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent Res J (Isfahan) 2015; 12:1-13.
- Lemongello GJ Jr: Fiber – Reinforced Bridge Replacement for Congenitally Missing Lateral Incisor. Contemp Esthet Restor Pract 2001; 2:1-4.
Author: Dentist Michał Godula
Graduate of the Pomeranian Medical University in Szczecin. Specialist Dental Center AHF Frelich in Żory. Head of Department: Dr. n. med. Henryk Frelich
Article published in issue 7/2022 of Nowy Gabinet Stomatologiczny magazine. See full table of contents.
Implantoprosthetic treatment of a patient with agenesis of the upper left lateral incisor – case report
Typografia
- Najmniejsza Mała Średnia Większa Największa
- Obecna Helvetica Segoe Georgia Times
- Tryb czytania