

AUTHORS: Agnieszka Cegłowska, Katarzyna Nowak
KEY WORDS: mosiodens, supernumerary teeth, impacted teeth, CBCT, surgical
ABSTRACT: Mesiodens is the most frequent form of supernumerary teeth. Its presence can cause various types of functional or anatomical disorders in the oral cavity, as well as be asymptomatic. Our work is based on a review of the literature and a case report of a patient admitted to the Dental Surgery Clinic of the Medical Center of the Medical University of Warsaw, Dentistry Department due to pain symptoms in the anterior jaw. Radiological diagnostics revealed incorrect endodontic treatment and a damaged follicle of the supernumerary tooth. The aim of the article is to draw the attention of physicians to the need to individually consider treatment methods depending on the patient's age and, above all, the symptoms of supernumerary teeth treatment .
ARTICLE PUBLISHED: March 24, 2023
Introduction
Hyperdontia refers to an increased number of teeth in the permanent or deciduous dentition and is caused by hyperactivity of the dental lamina, occurring sporadically or genetically (1). These teeth can take the form of supplemental teeth (with eumorphic – normal morphology) or supernumerary teeth (dysmorphic – abnormal morphology) (2). One of the most common types is mesiodens – a central supernumerary tooth that accounts for about half of all supernumerary teeth. It occurs in the midline, most often as a single tooth, in about 20% of cases in pairs or triplets (2), much more frequently in the maxilla than in the mandible (5, 6) – in the latter case, it is referred to as a mandibular mesiodens (Latin: hamulus) (4), with a male predilection (1). It most commonly has a conical or tuberculate form, more rarely rose-shaped, droplet-shaped, peg-shaped, stump-shaped, or with additional cusps (2). Radiological diagnostics of supernumerary teeth is based on conventional radiography, while for impacted teeth, cone-beam computed tomography (CBCT) is the method of choice. CBCT allows for precise localization, including the relationship to bony structures such as the floor of the nasal cavity (with perforation or preservation of the cortical plate), the nasopalatine canal (partial or complete location within the canal), and the external cortical plate of the alveolar process of the maxilla (3).
Case report
A 40-year-old female patient reported to the Dental Surgery Outpatient Clinic due to increasing pain in the midline region of the alveolar process of the maxilla. She reported trauma to the incisors followed by root canal treatment of tooth 11 about six months earlier. Radiological diagnostics, including maxillary CBCT, revealed the presence of a supernumerary tooth – mesiodens – and an improperly filled root canal of tooth 11. In this case, the position of the mesiodens corresponded to type IV according to Lin et al. It had an inverted conical shape, with the crown directed toward the nasal cavity and perforation of the cortical plate of its floor.
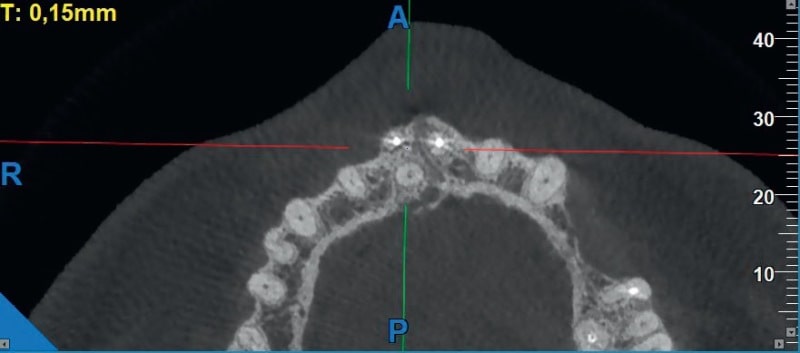
Fig. 1. Mesiodens located above the apices of the incisors

Fig. 2. Perforation of the cortical plate of the floor of the nasal cavity
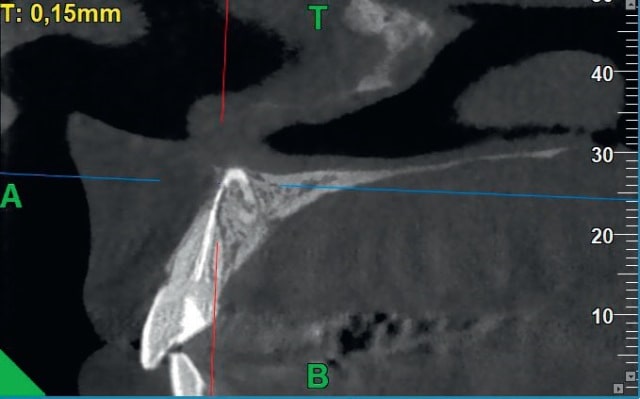
Fig. 3. Damage to the dental follicle of the mesiodens by a gutta-percha point
The endodontic material (gutta-percha point) located beyond the apex of the tooth damaged the follicle of the supernumerary tooth situated above. Consequently, surgical treatment was decided. Prior to the procedure, blood was drawn from the patient, and platelet-rich fibrin (PRF) was obtained by centrifugation. Under local infiltration anesthesia (Articaine hydrochloride 40 mg/ml + Adrenaline tartrate 0.01 mg/ml), a trapezoidal mucoperiosteal flap was raised with a marginal incision through the interdental papillae on the labial side of the alveolar process of the maxilla. The cortical bone of the process was removed using a surgical handpiece with a rose bur, and the excess endodontic material was removed with a slight apicoectomy of tooth 11 (retrograde filling with ProRoot MTA). The supernumerary tooth along with its follicle was then removed using luxation movements. PRF was placed in the postoperative bone cavity, the vestibular flap was repositioned, and the wound was sutured with single interrupted sutures (5/0 polyamide thread). The patient returned after 10 days for suture removal – proper healing of the soft tissues was observed. A follow-up visit was conducted after three months. Radiological examination (RVG) showed signs of proper bone tissue regeneration. The patient reported no complaints.
Discussion and conclusions
Impacted supernumerary teeth should be removed if they present anatomical or functional obstacles, or if they have an atypical appearance. They may cause retention of primary teeth, delayed, impacted, or ectopic eruption of permanent teeth, crowding, displacement, rotation of adjacent teeth, diastema, formation of primordial or follicular cysts, root resorption of adjacent teeth, and neuralgic pain. When located in the anterior region, they may also pose an aesthetic problem (2). In the case of unerupted central incisors where a mesiodens is an obstacle to their proper eruption, the removal of the supernumerary tooth should be performed as early as possible, ideally between the ages of 8 and 12, so that the force of spontaneous eruption of the tooth is used (9). The presence of impacted teeth that do not cause any disorders or complaints is not an indication for surgical intervention (7). Surgical removal of deeply located impacted teeth can cause significant bone tissue defects, may be associated with the need to extract other teeth (7) and the risk of damaging adjacent anatomical structures. The decision on therapeutic procedure should also take into account the patient's age - in people over 35 years of age, asymptomatic supernumerary teeth are left for observation (7). The case described by us concerns a patient above this age limit. However, the decision to remove the impacted tooth was dictated by damage to the dental follicle by a gutta-percha pin. Due to the significant invasiveness of the procedure related to the location of the supernumerary tooth - type IV according to Lin et al. (3), perforation of the compact plate of the nasal cavity floor - in order to improve the healing of soft tissues and bone tissue regeneration, platelet-rich fibrin (PRF) was used (8).
 Fig. 4. Trapezoidal mucoperiosteal flap with incision through the dental papilla.
Fig. 4. Trapezoidal mucoperiosteal flap with incision through the dental papilla.
 Fig. 5. Access to the supernumerary tooth is shown.
Fig. 5. Access to the supernumerary tooth is shown.
 Fig. 6. Removed messiodens
Fig. 6. Removed messiodens
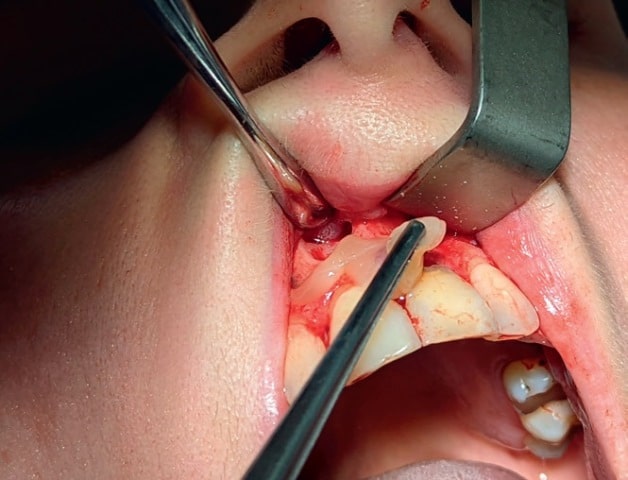 Fig. 7. Application of cell-rich fibrin (PRF)
Fig. 7. Application of cell-rich fibrin (PRF)
 Fig. 8. Suturing the wound with single knotted sutures.
Fig. 8. Suturing the wound with single knotted sutures.
Tab. 1. Classification of the position of supernumerary teeth in the anterior maxilla according to Lin et al.Type I Teeth located palatally in relation to the long axis of the adjacent normal incisor and below its apex Type II Teeth located palatally and above the apex of the adjacent normal incisor Type III Teeth located at the neck of normal teeth (in correct or reverse orientation) Type IV Teeth located above the tops of the adjacent incisors or obliquely (with the crown facing down or up) Type V The least numerous; teeth located labially in relation to the incisors Type VI Intermediate cases between types I and II |
The clinical case presented in this article illustrates the need to individualize surgical treatment methods. In the described patient, for many years, mesiodens did not cause disorders in the stomatognathic system. The incisors were properly erupted and positioned in the dental arch. Only trauma and improper root canal treatment led to damage to the supernumerary tooth follicle, which determined the need to remove it.
LITERATURE:
1. Cameron A., Widmer R., Kaczmarek U.; Pediatric Dentistry; Edra Urban & Partner, Wrocław 2012; 229–233;
2. Olczak-Kowalczyk D.; Szczepańska J.; Kaczmarek U.; Med Tour Press International; 1st ed., Otwock 2017; 138–139
3. Różyłło-Kalinowska I., Różyłło TK; Publishing House CZZąELEJ; 3rd Edition, Lublin 2021; 172–174;
4. Chęciński MA, Rubinkiewicz A, Chęcińska K. The mandibular median b – a review of the literature. Nowa Stomatol 2019; 24 (4): 127–132
5. Kaczmarek U.; Developmental abnormalities of teeth [in:] Jańczuk Z, Kaczmarek U, Lipski M (eds.). Conservative dentistry with endodontics. Clinical outline. 4th ed. PZWL, Warsaw 2014; 77–110
6. Trankmann J.; Development of dentition and occlusion [in:] Diedrich P (ed.). Orthodontics and development of oral-facial structures and diagnostics. Edra Urban & Partner, Wrocław 2004; 47–72
7. Dominiak M., Zapała J., Gedrange T.; Fundamentals of Oral Surgery. 2nd Expanded Edition, Edra Urban & Partner, Wrocław 2013; 224
8. Al- Maawi S., Becker K., Shwartz F., Sader R., Ghanaati S., Efcacy of platelet rich fbrin in promoting the healing of extraction sockets: a systematic review International Journal of Implant Dentistry (2021) 7:117
9. Kryst L. Maxillofacial surgery, PZWL Warsaw 1983; 106
Authors: DENTIST KATARZYNA NOWAK
Graduate of the Medical University of Warsaw. Currently specializing in dental surgery. Graduate of the Medical University of Warsaw. Currently specializing in dental surgery.
DENTAL DOCTOR AGNIESZKA CEGŁOWSKA
Graduate of the Medical University of Warsaw. Currently specializing in dental surgery.

